Disorders
Retinal detachment Retina
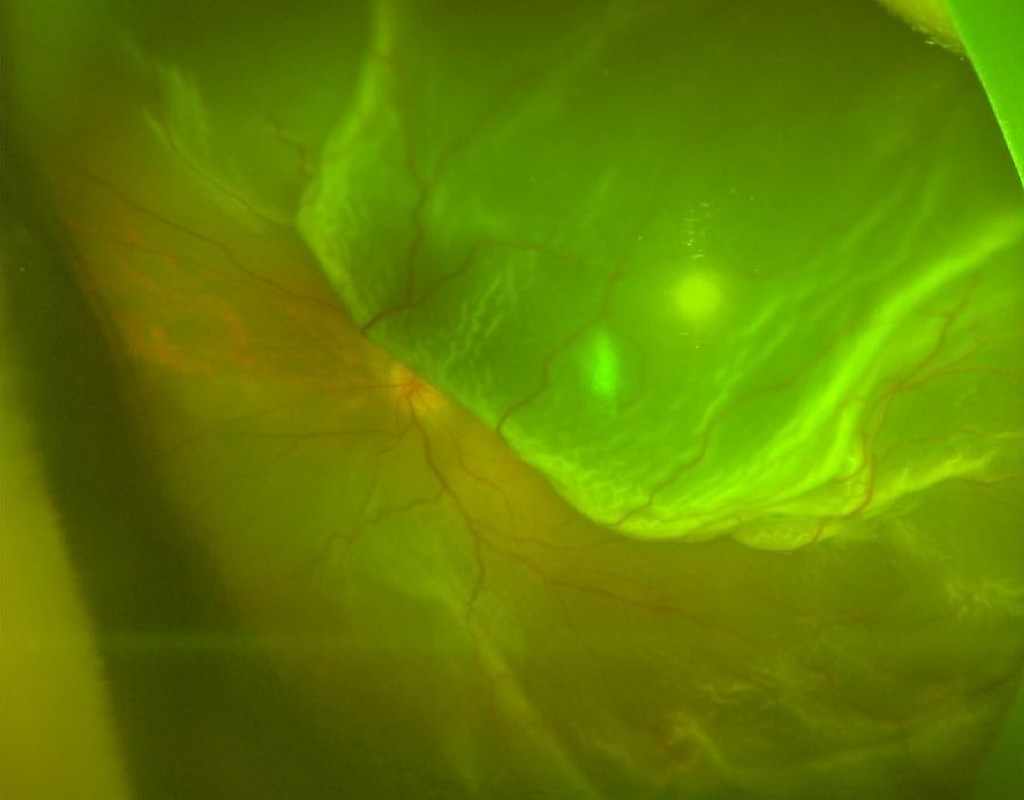
What is Retinal Detachment?
Retinal detachment consists of the separation of the neuro-sensory retina from the pigmented epithelium. It is a serious visual problem that can occur at any age but it usually strikes individuals from middle age. It is most common in people who are myopic or who have had a problem with the retina.
Epidemiology
Retinal detachment affects one in 10,000 people per year.
What are the causes?
Most retinal detachments are caused by the presence of one or more tears in the retinal structure. The vitreous is a transparent gel that is in contact with the retina on most of its surface, being more adherent in some anatomical areas. This gelatinous structure undergoes rheological changes with age, which induce the posterior detachment of the vitreous. Most vitreous detachments occur naturally and do not cause structural damage to the retina. However, retinal tears appear in some patients. Traction of the vitreous at these specific locations can cause a tear or a hole in the retina, through which the vitreous humor enters, inducing retinal detachment and subsequent evolution of the retina. In other cases, such as myopia, an inflammatory process or ocular trauma, posterior detachment of the vitreous can condition one or more retinal tears.
What are the symptoms of retinal detachment?
The most prevalent initial symptom is the perception of floating structures, called "flying flies" (myodesis) and light flashes (photophores). They may have the form of dots, lines or fragments in spider webs, which fluctuate and interfere objectively with our vision. In the case of progression of detachment, patients observe a shadow in the peripheral visual field (dark curtain). The retinal detachment will progressively reach the central vision and create a significant loss of vision if it is not diagnosed and treated quickly and effectively.
How is retinal detachment treated?
In the initial stage, if the retina presents a solution of continuity (tearing) but does not present clinical detachment, the detachment can be prevented through the early treatment with LASER photocoagulation. Once the subclinical tear and / or detachment develops, the treatment will always be surgical, in order to reapply the retina. The anatomic and functional postoperative prognosis is directly related to the evolution time of the detachment. Surgery performed may be at the endocular level (vitrectomy) or include an external approach (placement of scleral indentation).
Can we avoid retinal detachment?
It is important that people with myopia or relatives of people who have had a retinal detachment perform periodic eye exams by a retinal specialist so that early detection of predisposing peripheral retinal lesions is performed. It is also important to evaluate the contralateral eye in patients who have already had retinal detachment.
The sudden appearance of flying flies (myodesis) or a sudden increase of those that already exist, as well as the appearance of luminous flashes should be cause for quick reference for your ophthalmologist or for an Ophthalmological Emergency Service.
Request for Consultation
Make your online request here.
1st Consultation - € 85 and following € 80
Genetic Consultation - €90 (Private only)
See our Agreements and Partnerships!